We saw 2 patients yesterday that both had significant RVH
One had chest pain, the other had COPD exacerbation.
Can you pick which one had the ischaemia?
See the ECG#8 here for an infarct hiding in LBBB
See the ECG#8 here for an infarct hiding in LBBB






1 Comment
OK
so both these ECGs have RVH
.
The key to looking for ischaemia is knowing what the ST segments should be doing.
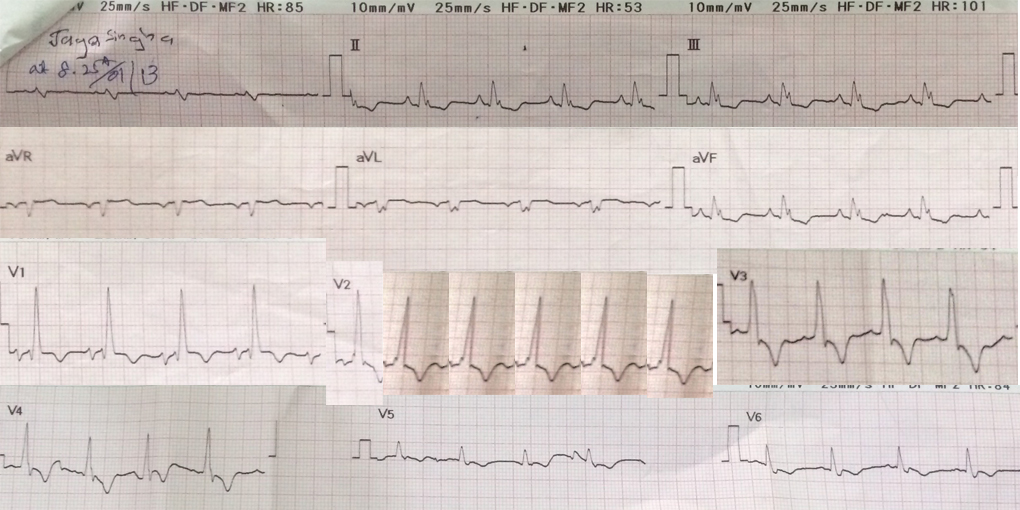
In RVH ST-T changes are opposite to the main QRS force direction. In the second ECG, you can see lots of TW inversion and sloping ST depression associated with tall R waves – this is the RVH strain patter that you see with more significant pulmonary hypertension.
.
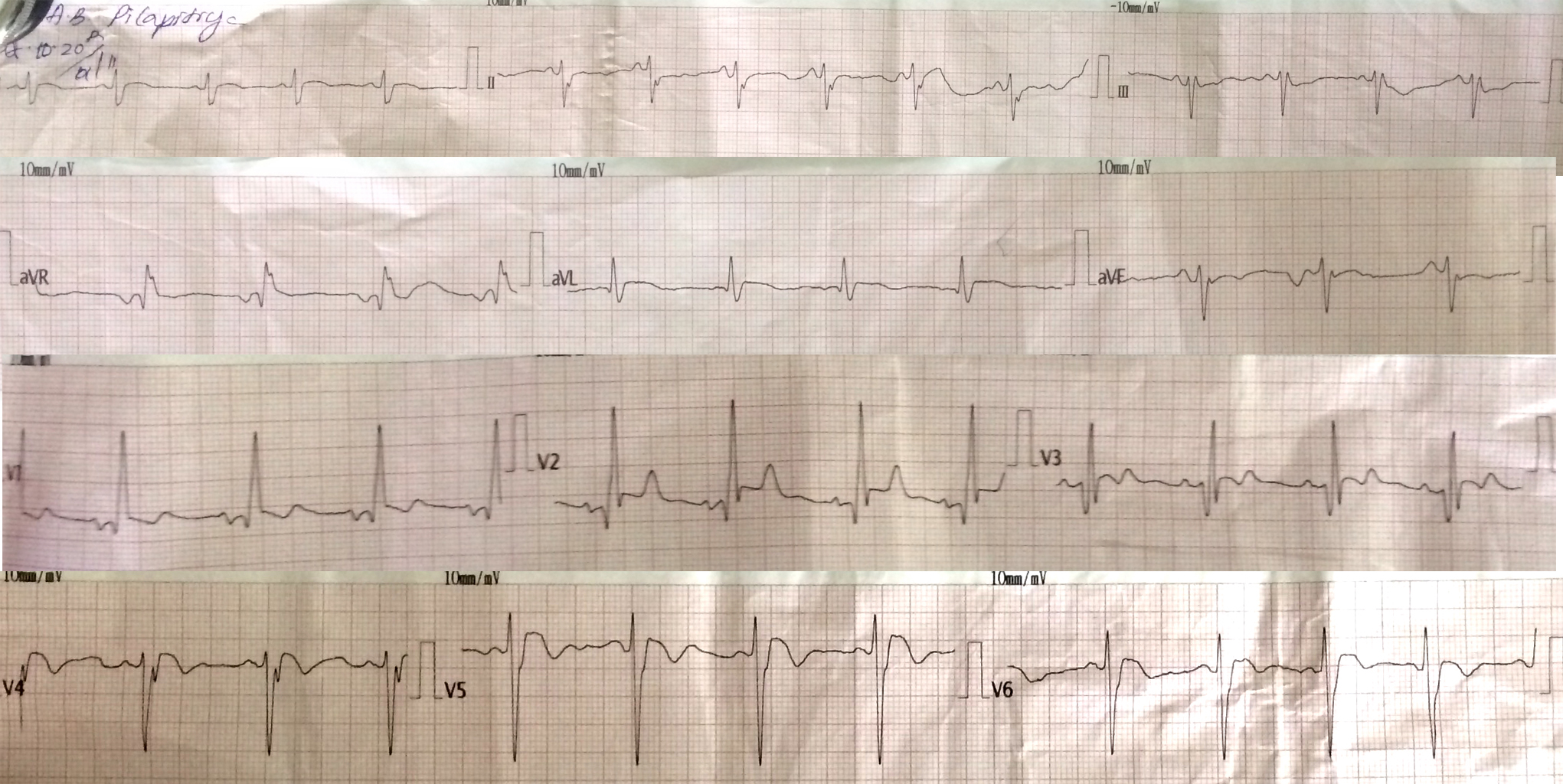
In the first ECG, the ST segments are elevated despite the R wave dominance – this is abnormal and is thus evidence of AMI. The patient became very unwell and developed cariogenic shock due to severe septal hypokinesis. This with some more experience might see the rounded appearance of the STE in V4-5 with biphasic TWs, which you often see in an infarct that is at least a few hours old.
.
Definitions of RVH are below, and come from the fabulous online ECG site ECG Learning Centre http://ecg.utah.edu
Right axis deviation (> 90 degrees)
Tall R-waves in RV leads; deep S-waves in LV leads
Slight increase in QRS duration
ST-T changes directed opposite to QRS direction (i.e., wide QRS/T angle)
May see incomplete RBBB pattern or qR pattern in V1
Evidence of right atrial enlargement (RAE) (lessonVII)
.
Specific ECG features (assumes normal calibration of 1 mV = 10 mm):
.
Any one or more of the following (if QRS duration < 0.12 sec): Right axis deviation (> 90 degrees) in presence of disease capable of causing RVH
R in aVR ≥ 5 mm, or
R in aVR > Q in aVR
Any one of the following in lead V1:
R/S ratio > 1 and negative T wave
qR pattern
R gt; 6 mm, or S < 2mm, or rSR' with R' > 10 mm
Other chest lead criteria:
R in V1 + S in V5 (or V6) 10 mm
R/S ratio in V5 or V6 < 1 R in V5 or V6 < 5 mm S in V5 or V6 > 7 mm
ST segment depression and T wave inversion in right precordial leads is usually seen in severe RVH such as in pulmonary stenosis and pulmonary hypertension.