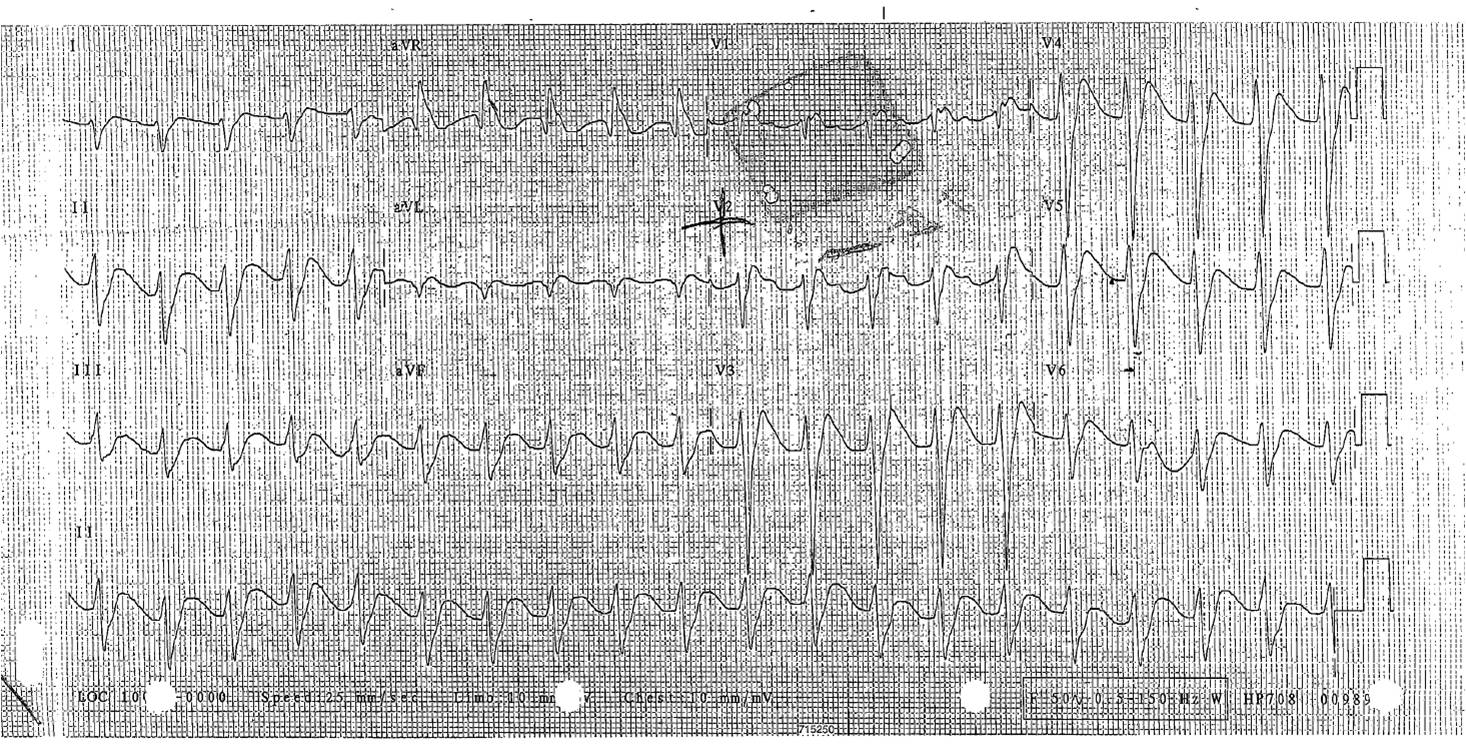
Well done Ilhaam, this ECG does show classic features of Sodium channel blocker OD, the most common of which are tricyclic antidepressants.
The key features are the wide QRS, long QT and tall R waves in aVR. The nuance here is that due to the anticholinergic effects of TCA, you often have a more significant tachycardia when toxic.
This is actually a Propranolol OD and its main CVS Fx are Na+ channel blocking not B blockade in overdose.
.
The rhythm is tricky and is probably a sino ventricular rhythm, Im not convinced I can see p waves although you could argue they are cojoined with the t wave.
Hyperkalaemia also causes a sino ventricular rhythm (where the sinus node is generating an impulse but the p wave is not visible) and as the ECG morphs into a sine wave it can look like this.
.
From a management perspective , a presentation such as this should scare you big time . I would advocate an aggressive pre emptive approach. Fitting and this ECG = bad. The resp acidosis during an RSI may be the trigger for arrhythmias (which are the trigger for more acidosis etc etc). but waiting for another fit or arrythmia before ETT is a recipe for disaster.
I would pre O2, avoid sedation prior ( no BZD), monitor on lead aVR (you can change the lead on the monitor) . Just prior to intubation I would give a bicarb load of 100mmol, and throw in a stat saline bag, gently hand bag during the induction phase and hyperventilate post tube.
I would probably give intralipid at the first sign of ECG worsening, there is case based support and best bets had this to say:
“There are no human studies about the use of intravenous lipid emulsion in β-blocker overdose. Studies on rodents and rabbits have shown that intralipid reduces QRS duration and improves bradycardia and hypotension in propranolol toxicity. Similar studies with metoprolol failed to show a significant improvement in blood pressure. Intravenous lipid emulsion is thought to act as a lipid sink, attracting the drugs away from tissues, and thus may be more effective with more lipophilic drugs such as propranolol compared with metoprolol. Several case reports provide anecdotal suggestions of benefit but no firm evidence is available and it is likely that there is publication bias. Intravenous lipid emulsion has recently been recommended by Toxbase as worth consideration in patients with a history of overdose of β blockers, who have cardiotoxic symptoms that are not responsive to standard treatment.(Toxbase)”
.
As stated the R wave ration in aVR is important, although like most things in tox the PPVs are not great. incidentally a study which brought aVR to prominence was done in the Canberra Hospital see below
Abstract
Objective
The aim of the present study was to examine the relationship between serious arrhythmias in patients with psychotropic drug overdose and electrocardiography (ECG) findings that have been suggested previously to predict this complication.
Methods
Thirty-nine patients with serious arrhythmias (ventricular tachycardia, supraventricular tachycardia or cardiac arrest) after tricyclic antidepressant overdose or thioridazine overdose were compared with 117 controls with clinically significant overdose matched to each case for the drug ingested. These patients with psychotropic drug overdose had presented for treatment to the Department of Clinical Toxicology, Newcastle and to the Princess Alexandra Hospital, Brisbane. The heart rate, the QRS width, the QTc and QT intervals, the QT dispersion, and the R wave and R/S ratios in aVR on the initial ECGs were compared in cases and controls.
Results
The cases had taken dothiepin (16 patients), doxepin (six patients), thioridazine (five patients), amitriptyline (five patients), nortriptyline (three patients), imipramine (one patient) and a combination of dothiepin and thioridazine (three patients). In 20 of the 39 patients with arrhythmias, the arrhythmia had been a presumed ventricular tachycardia. Of the other 19 patients, 15 patients had a supraventricular tachycardia, two patients had cardiac arrests (one asystole, one without ECG monitoring) and two patients had insufficient data recorded to make classification of the arrhythmias possible. The QRS was ≥ 100 ms in 82% of cases but also in 76% of controls. QRS ≥ 160 ms had a sensitivity of only 13% and occurred in 2% of controls. QRS > 120 ms, QTc > 500 and the R/S ratio in aVR appeared to have a stronger association with the occurrence of arrhythmia: QRS > 120 ms (odds ratio [OR], 3.56; 95% confidence interval [CI], 1.46–8.68), QTc > 500 (OR, 3.07; 95% CI, 1.33–7.07), and R/S ratio in aVR > 0.7 (OR, 16; 95% CI, 3.47–74). Excluding thioridazine overdoses and performing the analysis for tricyclic antidepressant overdoses alone gave increased odds ratios for QRS > 120 ms (OR, 4.83; 95% CI, 1.73–13.5) and QTc > 500 (OR, 4.5; 95% CI, 1.56–13) but had little effect on that for the R/S ratio in aVR > 0.7 (OR, 14.5; 95% CI, 3.10–68).
Conclusion
ECG measurements were generally weakly related to the occurrence of arrhythmia and should not be used as the sole criteria for risk assessment in tricyclic antidepressant overdose. The frequently recommended practice of using either QRS ≥ 100 ms or QRS ≥ 160 ms to predict arrhythmias is not supported by our study. R/S ratio in aVR > 0.7 was most strongly related to arrhythmia but had estimated positive and negative predictive values of only 41% and 95%, respectively. The use of these specific predictors in other drug overdoses is not recommended without specific studies.
The limited utility of electrocardiography variables used to predict arrhythmia in psychotropic drug overdose
Nicholas A Buckley1*, Stephan Chevalier2, I Anne Leditschke3, Dianne L O’Connell4, James Leitch5 and Susan M Pond
Critical Care 2003, 7:R101-R107






2 Comments
Widen qrs complex in aVR with prolonged QT interval, seizures suggestive of TCA overdose
Management
Airway protection needs intubation GCS 6
VBG
NaHCO3
ICU admission
Psych team review
Well done Ilhaam, this ECG does show classic features of Sodium channel blocker OD, the most common of which are tricyclic antidepressants.
The key features are the wide QRS, long QT and tall R waves in aVR. The nuance here is that due to the anticholinergic effects of TCA, you often have a more significant tachycardia when toxic.
This is actually a Propranolol OD and its main CVS Fx are Na+ channel blocking not B blockade in overdose.
.
The rhythm is tricky and is probably a sino ventricular rhythm, Im not convinced I can see p waves although you could argue they are cojoined with the t wave.
Hyperkalaemia also causes a sino ventricular rhythm (where the sinus node is generating an impulse but the p wave is not visible) and as the ECG morphs into a sine wave it can look like this.
.
From a management perspective , a presentation such as this should scare you big time . I would advocate an aggressive pre emptive approach. Fitting and this ECG = bad. The resp acidosis during an RSI may be the trigger for arrhythmias (which are the trigger for more acidosis etc etc). but waiting for another fit or arrythmia before ETT is a recipe for disaster.
I would pre O2, avoid sedation prior ( no BZD), monitor on lead aVR (you can change the lead on the monitor) . Just prior to intubation I would give a bicarb load of 100mmol, and throw in a stat saline bag, gently hand bag during the induction phase and hyperventilate post tube.
I would probably give intralipid at the first sign of ECG worsening, there is case based support and best bets had this to say:
“There are no human studies about the use of intravenous lipid emulsion in β-blocker overdose. Studies on rodents and rabbits have shown that intralipid reduces QRS duration and improves bradycardia and hypotension in propranolol toxicity. Similar studies with metoprolol failed to show a significant improvement in blood pressure. Intravenous lipid emulsion is thought to act as a lipid sink, attracting the drugs away from tissues, and thus may be more effective with more lipophilic drugs such as propranolol compared with metoprolol. Several case reports provide anecdotal suggestions of benefit but no firm evidence is available and it is likely that there is publication bias. Intravenous lipid emulsion has recently been recommended by Toxbase as worth consideration in patients with a history of overdose of β blockers, who have cardiotoxic symptoms that are not responsive to standard treatment.(Toxbase)”
.
As stated the R wave ration in aVR is important, although like most things in tox the PPVs are not great. incidentally a study which brought aVR to prominence was done in the Canberra Hospital see below
Abstract
Objective
The aim of the present study was to examine the relationship between serious arrhythmias in patients with psychotropic drug overdose and electrocardiography (ECG) findings that have been suggested previously to predict this complication.
Methods
Thirty-nine patients with serious arrhythmias (ventricular tachycardia, supraventricular tachycardia or cardiac arrest) after tricyclic antidepressant overdose or thioridazine overdose were compared with 117 controls with clinically significant overdose matched to each case for the drug ingested. These patients with psychotropic drug overdose had presented for treatment to the Department of Clinical Toxicology, Newcastle and to the Princess Alexandra Hospital, Brisbane. The heart rate, the QRS width, the QTc and QT intervals, the QT dispersion, and the R wave and R/S ratios in aVR on the initial ECGs were compared in cases and controls.
Results
The cases had taken dothiepin (16 patients), doxepin (six patients), thioridazine (five patients), amitriptyline (five patients), nortriptyline (three patients), imipramine (one patient) and a combination of dothiepin and thioridazine (three patients). In 20 of the 39 patients with arrhythmias, the arrhythmia had been a presumed ventricular tachycardia. Of the other 19 patients, 15 patients had a supraventricular tachycardia, two patients had cardiac arrests (one asystole, one without ECG monitoring) and two patients had insufficient data recorded to make classification of the arrhythmias possible. The QRS was ≥ 100 ms in 82% of cases but also in 76% of controls. QRS ≥ 160 ms had a sensitivity of only 13% and occurred in 2% of controls. QRS > 120 ms, QTc > 500 and the R/S ratio in aVR appeared to have a stronger association with the occurrence of arrhythmia: QRS > 120 ms (odds ratio [OR], 3.56; 95% confidence interval [CI], 1.46–8.68), QTc > 500 (OR, 3.07; 95% CI, 1.33–7.07), and R/S ratio in aVR > 0.7 (OR, 16; 95% CI, 3.47–74). Excluding thioridazine overdoses and performing the analysis for tricyclic antidepressant overdoses alone gave increased odds ratios for QRS > 120 ms (OR, 4.83; 95% CI, 1.73–13.5) and QTc > 500 (OR, 4.5; 95% CI, 1.56–13) but had little effect on that for the R/S ratio in aVR > 0.7 (OR, 14.5; 95% CI, 3.10–68).
Conclusion
ECG measurements were generally weakly related to the occurrence of arrhythmia and should not be used as the sole criteria for risk assessment in tricyclic antidepressant overdose. The frequently recommended practice of using either QRS ≥ 100 ms or QRS ≥ 160 ms to predict arrhythmias is not supported by our study. R/S ratio in aVR > 0.7 was most strongly related to arrhythmia but had estimated positive and negative predictive values of only 41% and 95%, respectively. The use of these specific predictors in other drug overdoses is not recommended without specific studies.
The limited utility of electrocardiography variables used to predict arrhythmia in psychotropic drug overdose
Nicholas A Buckley1*, Stephan Chevalier2, I Anne Leditschke3, Dianne L O’Connell4, James Leitch5 and Susan M Pond
Critical Care 2003, 7:R101-R107