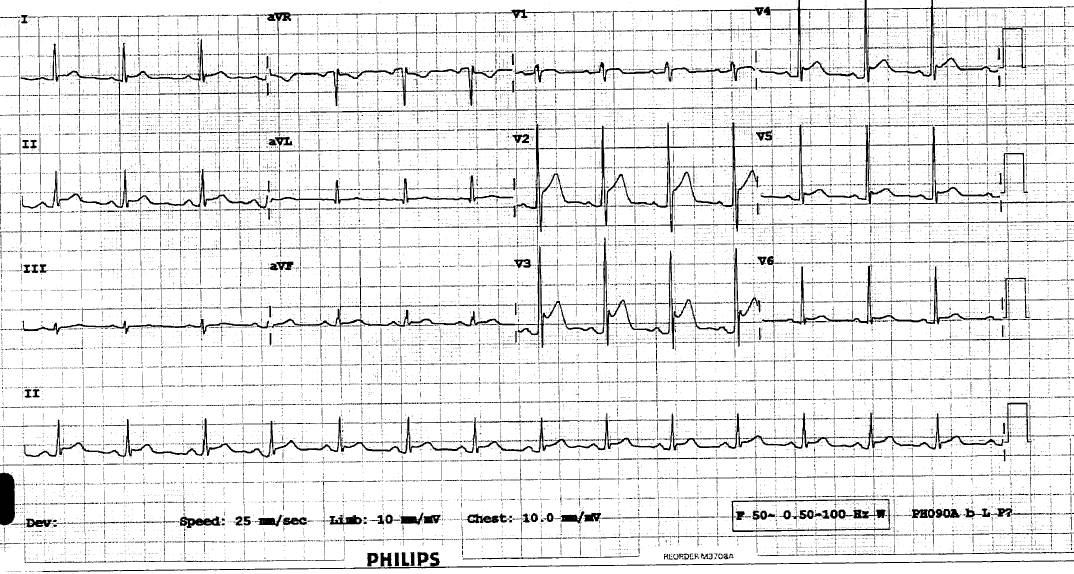
The most concerning feature here is ST elevation in a male smoker with chest pain.
Morphology of ST elevation is very important however,and this STE is concave upsloping and also is found in more than one artery territory. In general ischaemic STE is horizontal and confined to a single artery (with reciprocal changes (usually of ST depression) seen in the leads opposite to the main area of damage).
.
Given the shape of the STE and the widespread change and PR depression; : the most likely diagnosis is pericarditis but DDX and watch for; AMI
Remember that ECG changes in pericarditis are due to inflammation and damage to the epicardial layer of the myocardium, so all pericarditis with ECG findings have myocardial involvement…hence sometimes the very gnarly looking ECGs..the more myocardial involvement, the ‘worse’ the ECG looks.
.
This patient had more classic pericarditis pain earlier but developed more ischaemic tightness in ED. We sent him for urgent coronary angio as his STE was evolving rapidly, but thankfully he had normal vessels.
So Management would be analgesia, try GTN, give aspirin, hold off enoxaparin and get urgent cardiology opinion re diagnostic angio if uncertain. A bedside echo showing small pericardial effusion may be helpful, but is not specific enough to ‘diagnose’ pericarditis and exclude ischaemia. Troponin will be elevated in both epicarditis and AMI, usually less high in epicarditis






1 Comment
The most concerning feature here is ST elevation in a male smoker with chest pain.
Morphology of ST elevation is very important however,and this STE is concave upsloping and also is found in more than one artery territory. In general ischaemic STE is horizontal and confined to a single artery (with reciprocal changes (usually of ST depression) seen in the leads opposite to the main area of damage).
.
Given the shape of the STE and the widespread change and PR depression; : the most likely diagnosis is pericarditis but DDX and watch for; AMI
Remember that ECG changes in pericarditis are due to inflammation and damage to the epicardial layer of the myocardium, so all pericarditis with ECG findings have myocardial involvement…hence sometimes the very gnarly looking ECGs..the more myocardial involvement, the ‘worse’ the ECG looks.
.
This patient had more classic pericarditis pain earlier but developed more ischaemic tightness in ED. We sent him for urgent coronary angio as his STE was evolving rapidly, but thankfully he had normal vessels.
So Management would be analgesia, try GTN, give aspirin, hold off enoxaparin and get urgent cardiology opinion re diagnostic angio if uncertain. A bedside echo showing small pericardial effusion may be helpful, but is not specific enough to ‘diagnose’ pericarditis and exclude ischaemia. Troponin will be elevated in both epicarditis and AMI, usually less high in epicarditis